If you have symptoms of a thyroid disorder and thyroid tests are normal, the symptom is not your thyroid. There are many conditions that have symptoms that overlap with thyroid disease, so it is better to look for the cause instead of just blaming the thyroid.
There is a bidirectional relationship between thyroid hormones and fatty liver. NAFLD causes decreased thyroid hormone signaling which can then lead to worsening of a fatty liver.
Don’t fall for functional medicine thyroid gaslighting and focus on established treatments for fatty liver disease.
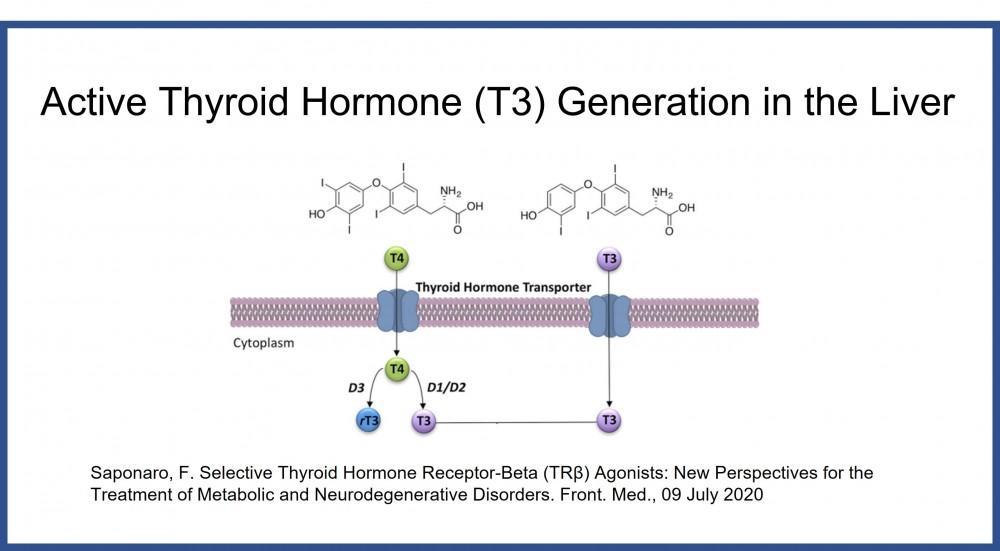
Thyroid hormones are shunted to inactive reverse T3 in fatty liver disease when deiodinase-3 prevails over deiodinase-1 in an injured liver. Thyroid hormone activity is controlled by hepatic deiodinases. Expressions of D1 & D3 are altered in an injured fatty liver leading to increased reverse T3 and intrahepatic hypothyroidism. Fat in hepatocytes causes inflammation by increasing IL-6 & TNF-α and pro-oxidative effects. This can decrease liver D1 activity (decreasing T4->T3 conversion) and increase liver D3 activity (increasing inactivation of T4->rT3).
Decreasing plasma free T4 levels are associated with an increasing prevalence and worsening of NAFLD in type 2 diabetes. Low-normal thyroid function within the euthyroid reference range increases cholesterol, triglycerides and insulin resistance which may contribute to the pathogenesis of atherosclerotic cardiovascular disease. There is a positive correlation between FT3/FT4 ratio and NAFLD and a negative relationship between FT4, TT3, and TT4 levels and risk of progressive hepatic fibrosis. The assessment of thyroid hormone levels within the normal range in patients with type 2 diabetes could be helpful in the prevention and treatment of NAFLD.
The management of hepatic hypothyroidism starts with getting fat out of the liver. Weight loss with a diet plan is helpful for patients that need to lose a lot of weight and have had difficulty doing it alone. Fast weight loss under medical supervision has been proven to work best because it is more motivating, compared to slow weight loss that can be frustrating.
Although there are no medications that have been officially approved to treat hepatic hypothyroidism, Resmetirom is entering the final states of testing as a treatment for more advanced forms of fatty liver disease. Resmetirom is a liver-directed, oral, thyroid hormone receptor-β agonist designed to improve liver health by increasing hepatic fat metabolism and reducing lipotoxicity. The drug works to try to overcome some of the effects of intrahepatic hypothyroidism by stimulating a thyroid hormone receptor located in the liver.
Treatments for nonalcoholic fatty liver disease starting with weight loss address the root cause of hepatic hypothyroidism by helping to heal a hypothyroid liver. Medications used to treat fatty liver disease include diabetes medications (such as GLP-1 medications tirzepatide - Mounjaro, semaglutide - Ozempic, Wegovy, Rybelsus or liraglutide-Saxenda, Victoza) and weight loss medications such as Qsymia or Contrave. Even better results can be obtained by using a combination of medications.
At Atlanta Endocrine Associates, Dr. Scott Isaacs is a fatty liver expert and offers accurate diagnosis and state-of-the-art treatment of thyroid disorders.