Bariatric surgery results in superior short-term and long-term weight loss outcomes and improvements in obesity-related comorbidities compared to non‐surgical treatments. At Atlanta Endocrine Associates, Dr. Scott Isaacs is a weight loss expert and offers accurate diagnosis and state-of-the-art weight management including Mounjaro (tirzepatide) and Wegovy (semaglutide). To learn more, contact the office in Atlanta, Georgia.
The amount of weight loss, regardless of modality, is associated with incremental improvements in comorbidities like type 2 diabetes, fatty liver disease, dyslipidemia, hypertension, and sleep apnea. The average weight loss for patients who undergo bariatric surgery is around 33% of initial body weight compared to an average weight loss of 10% with anti-obesity medications and 3-5% with a low-calorie diet and lifestyle modification. The superior outcomes and magnitude of weight loss have resulted in an increase in the number of bariatric procedures that have been performed in recent years. With increasing numbers of bariatric surgeries, weight regain, also known as weight recidivism, has emerged as a significant problem.
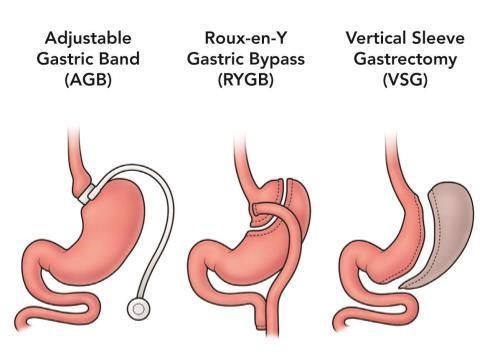
Bariatric surgery is indicated for chronic weight management in adult patients with an initial BMI of >40 kg/m2 or in adult patients with a BMI of >35 kg/m2 who have comorbidities of obesity such as type 2 diabetes, hypertension, or dyslipidemia. Sleeve gastrectomy restricts energy intake by reducing stomach size to a small pouch. Roux-en-Y gastric bypass is both a restrictive procedure as well as a malabsorptive procedure which limits the absorption of calories. Bariatric surgery is also referred to as metabolic surgery because it produces changes in the production of hunger and satiety hormones secreted by endocrine cells in the gut that signal the brain to reduce appetite and enhance satiation. Bariatric surgery is effective in maintaining long-term weight loss because the anatomical and biological changes allow continued energy restriction in the face of metabolic and hormonal adaptive changes known to occur with weight loss.
Weight recidivism is primarily a physiological process, and not the result of loss of will power. When weight is regained, the comorbidities that were present before weight loss are likely to reappear. Approximately one-third of patients will regain more than 25% of their initial weight loss within 2 to 5 years of surgery. One study found that over 40% of patients had regained weight 10 years after bariatric surgery. The best way to prevent recurrence of comorbidities is to recognize weight regain early enough to provide effective interventions to address to reverse or lessen weight regain.
The process of weight regain occurs when excess calories are consumed above metabolic requirements resulting in accumulation of body fat. Hormonal, behavioral, environmental, metabolic, anatomical, and surgical factors can contribute to excess calorie intake known as metabolic overfeeding.
Hormonal factors:
In the first six months after bariatric surgery, food intake is reduced significantly. Although the restriction of stomach size plays a key role, this effect is also attributed to alterations in satiety and hunger hormones, such as glucagon-like peptide 1 (GLP-1), cholecystokinin, peptide YY, ghrelin, pancreatic polypeptide, and leptin. After 12-24 months, the effect diminishes, leading to increased appetite and decreased satiety and resumption of overeating. Pharmacotherapy with anti-obesity medications has been identified as an effective way to address metabolic overfeeding. The same guidelines for pharmacotherapy with anti-obesity medications in non-surgical patients should be followed for bariatric surgery patients. Medication choice should be individualized to the patient according to contraindications, drug interactions and prior history of adverse effects. Start with the lowest dose and titrate as needed. If weight loss is not achieved with a single agent, the medication should be discontinued and initiation of a different medication. Combination treatments can be used when a single medication is ineffective.
Behavioral/environmental factors:
Disordered eating habits such as grazing, night eating, binge eating, eating a lot of soft foods (i.e., mashed potatoes or ice cream), high calorie beverages or other forms of disordered eating contribute to weight regain. Poor dietary choices with snack foods, fast foods and sweets can also be a factor. It is vital that patients are educated about postoperative diet, physical activity, and lifestyle behaviors necessary for achieving the best possible long-term outcomes. Even though extensive education is provided preoperatively, this requires lifelong follow-up post-operatively with a bariatric multidisciplinary team. Patients must maintain a diet that is low in calories and fat with high quality protein, at least 5 servings of vegetables and fruits and avoidance of sugars and refined carbohydrates. Liquid calories, including coffee drinks, juices, sugar sweetened beverages and alcohol should be minimized or avoided entirely. Specific limitations on food choices and eating behaviors are necessary due to altered anatomy of the GI tract. Limiting the portion size of meals to one-half cup per 30 minutes helps prevent stretching of the gastric pouch. Patients are encouraged to eat slowly, chew thoroughly, and avoid large volumes of food.
Metabolic factors:
Adaptive thermogenesis is a slowing of metabolic rate as a response to weight loss greater than what would be predicted by the weight loss itself. This metabolic adaptation is a biological survival mechanism that conserves energy in the face of starvation and dangerously low energy supplies. However, the contribution of adaptive thermogenesis is thought to be only about 50-100 kcal/day and lessens over time. A low carbohydrate diet may also help reduce the effects of adaptive thermogenesis after weight loss.
Surgical and anatomical factors:
Potential anatomical factors that can contribute to weight regain include dilation of the gastrojejunal stoma and distention of the gastric pouch. A less common surgical complication can be the development of a gastrogastric fistula resulting in communication between the proximal gastric pouch and the distal gastric remnant. An upper GI series is useful for diagnosis. Drinking fluids with meals can cause enlargement of the gastric pouch and outlet and leads to rapid emptying of the stomach. This can be avoided by instructing patients to delay fluid intake for at least 30 minutes after consuming a meal. Surgical and anatomical abnormalities can be corrected surgically or endoscopically, although rarely covered by third-party payers. With the increase in the number of patients undergoing a bariatric surgical procedure, weight recidivism has been recognized as a significant problem. Patients should have livelong monitoring and when weight regain does occur, it should be identified and addressed as early as possible. Weight recidivism is usually multifactorial, including anatomical, hormonal, metabolic, behavioral, and environmental factors. By educating patients preoperatively and with ongoing dietary and behavioral support, weight regain can be minimized or avoided. When necessary, pharmacotherapy can be used, and endoscopic or surgical revision procedures can be performed.
When the time is right, we are here for you. To get started, all you have to do is give us a call.